Bronchiolitis in babies: a guide for parents
Dr. Francisco Javier Recio Valcarce
As a home-visit pediatrician, I understand how distressing it can be to see your baby with respiratory symptoms. Below, I offer a clear and comprehensive explanation of what bronchiolitis is, how to recognize it, what care you can provide at home, and when it is essential to seek medical attention. This guide is intended for parents looking for reliable information.
What is bronchiolitis?
Bronchiolitis is a viral infection of the lower airways that mainly affects babies under 2 years of age, especially between 2 and 6 months.
The most common cause is the Respiratory Syncytial Virus (RSV), although other common respiratory viruses can also be responsible.
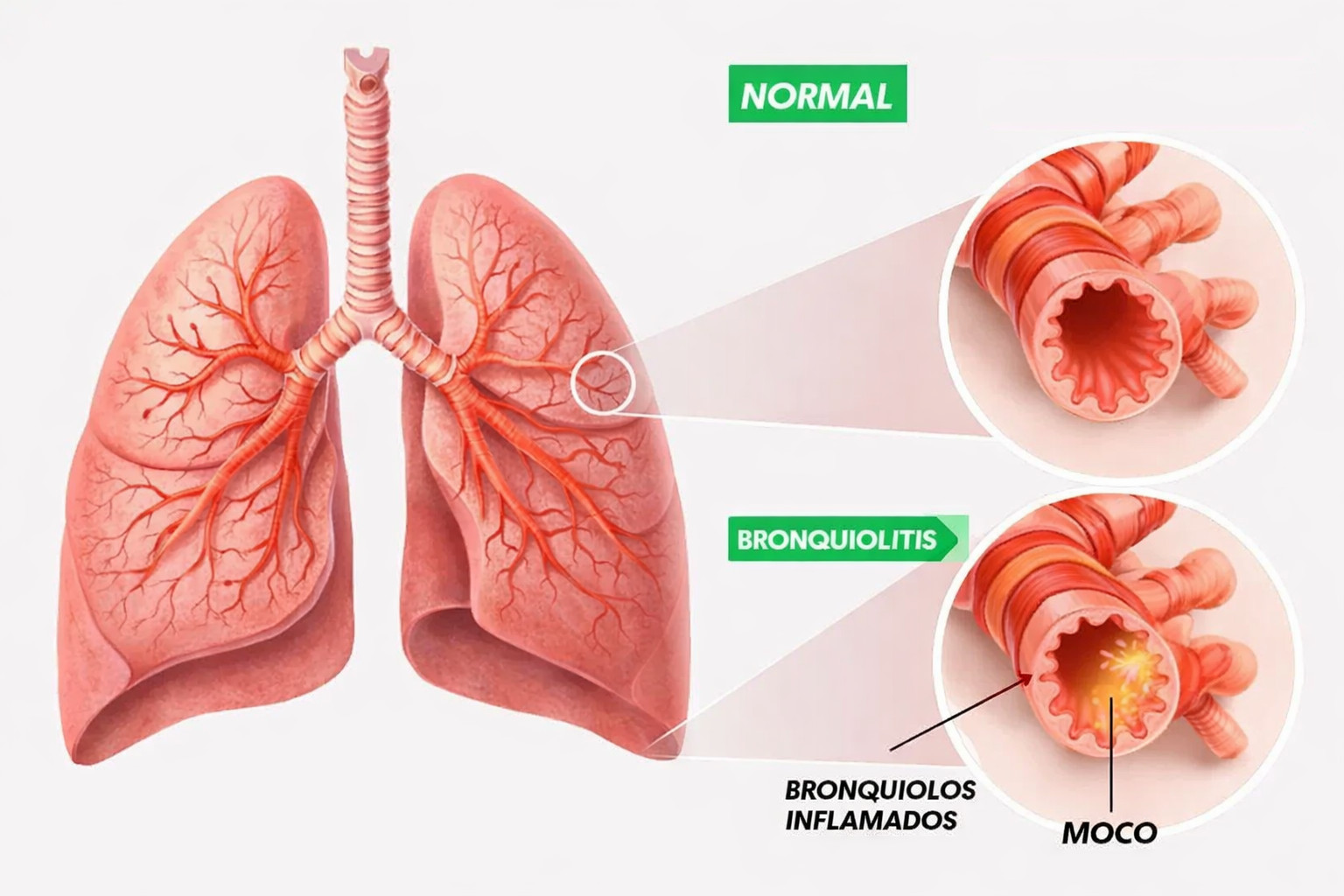
The infection causes inflammation, swelling, and increased mucus production in the bronchioles (the smallest airways in the lungs), making it harder for air to flow.
Bronchiolitis usually occurs during the autumn and winter months (in the Northern Hemisphere) or during the cold and rainy season.

What symptoms does bronchiolitis cause?
Parents may notice several signs that suggest bronchiolitis may be developing. It is important to watch for both mild symptoms and warning signs.
Bronchiolitis often begins with symptoms similar to a common cold. Paying attention to these early signs is crucial, as they can progress to a more serious condition.
Runny nose and nasal discharge: One of the first signs is usually a clear nasal discharge, which may become thicker and greenish over time. Constant runny nose indicates congestion of the upper airways.
Sneezing and nasal congestion: Frequent sneezing is an attempt to clear the nasal passages, while congestion makes breathing difficult—especially in babies who cannot blow their nose. This may cause noisy breathing.
Mild cough: At first, the cough may be dry and occasional. As the illness progresses, it often becomes wetter, more persistent, and may be accompanied by mucus.
Low-grade fever: High fever is not always present. Many babies with bronchiolitis have only a low-grade fever (usually between 37.5 °C and 38 °C), and some may have no fever at all. The absence of high fever does not rule out the infection.
Other symptoms that may help identify bronchiolitis include:
Reduced appetite or difficulty feeding: Nasal congestion and breathing difficulty can interfere with feeding, as babies struggle to coordinate sucking and breathing. This may result in shorter feeds, irritability during feeding, or refusal to eat.
Irritability: Infants may appear more irritable or restless due to general discomfort.
Changes in sleep patterns: Breathing difficulties and coughing can disrupt sleep, making the baby more tired during the day.
It is essential to monitor how these symptoms evolve and seek medical advice if they worsen or if signs of breathing difficulty appear, such as rapid breathing, nasal flaring, or chest retractions.
After 2–4 days, bronchiolitis may progress in some babies and begin to affect the bronchioles, the smallest airways in the lungs. This progression can cause symptoms that require closer attention:
Increased cough and congestion: The cough becomes more intense and persistent, and nasal and chest congestion worsen, making breathing more difficult.
Wheezing: A characteristic whistling sound may be heard when the baby breathes, especially when exhaling. Wheezing indicates narrowing of the airways.
Breathing difficulty: Breathing becomes faster and more labored. You may notice chest retractions, where the ribs or the area below the chest sink in during inhalation, showing increased effort to breathe.
Nasal flaring: The baby’s nostrils widen noticeably while breathing, an unconscious effort to take in more oxygen.
Poor feeding tolerance, sleepiness, or irritability: The increased effort of breathing can tire the baby quickly during feeds, leading to reduced intake. The baby may appear unusually sleepy and apathetic, or conversely, more irritable and unsettled.
Being alert to these signs is important, as they may indicate disease progression and the need for medical evaluation to ensure proper care and the baby’s well-being.
You should seek immediate medical attention if your child shows any of the following warning signs:
Bluish skin, lips, or fingernails (cyanosis): This indicates a lack of oxygen and is a medical emergency.
Breathing pauses (apnea), very rapid breathing, or severe breathing effort:
Apnea: Any prolonged pause in breathing is an emergency.
Very rapid breathing (tachypnea): Especially if accompanied by other symptoms, it may signal poor oxygenation.
Severe breathing effort: Use of neck or chest muscles, visible retractions between the ribs, nasal flaring, or grunting sounds suggest the child is struggling to breathe.
Very low fluid intake or few wet diapers (dehydration): Signs include minimal drinking, fewer wet diapers than usual, lethargy, dry mouth, absence of tears when crying, or sunken eyes.
Complete refusal to feed, lethargy, or progressive worsening:
Complete refusal to eat or drink for a significant period is concerning.
Lethargy: The child appears unusually sleepy, apathetic, low in energy, and less responsive.
Progressive worsening: If the child’s condition does not improve or continues to deteriorate—such as increasing fever, worsening breathing, or new concerning symptoms—medical attention is essential.
If any of these signs appear, do not hesitate to seek urgent medical care. Early detection and prompt treatment can be crucial for your child’s health.

Why does bronchiolitis occur and who is most at risk?
Babies are especially vulnerable to respiratory illnesses such as bronchiolitis. Their airways are smaller and narrower than those of adults, which means that inflammation or mucus buildup can block them more easily, making breathing significantly more difficult. In addition, their immune system is still immature, limiting their ability to effectively fight viruses and bacteria. As a result, infections can be more severe and last longer.
Several factors increase the risk of bronchiolitis becoming more severe in a baby:
Very young age: Babies under 3 to 6 months are the most vulnerable to serious complications. At this stage, their lungs are still developing and their immune system is particularly immature, making it harder for them to cope with the infection on their own.
Prematurity: Babies born prematurely have underdeveloped lungs and a weaker immune system, placing them at a significantly higher risk of severe bronchiolitis and other respiratory complications.
Underlying medical conditions: Babies with pre-existing conditions such as congenital heart disease, chronic lung disease (such as bronchopulmonary dysplasia), or a weakened immune system (due to medical treatments or genetic conditions) have a reduced ability to fight infection. In these cases, bronchiolitis can worsen their underlying condition and lead to more serious outcomes.
In addition to biological factors, a baby’s environment also plays an important role in the risk and severity of bronchiolitis:
Exposure to tobacco smoke: Secondhand smoke weakens a baby’s airways, making them more prone to respiratory infections and increasing the severity of bronchiolitis. Toxins in tobacco smoke irritate the lungs and impair ciliary function, which helps clear germs from the airways.
Crowded living conditions: Living in crowded environments increases the likelihood of respiratory virus transmission, as babies are in closer contact with people who may carry infections.
Daycare settings with poor hygiene: Environments without strict hygiene measures make it easier for germs to spread. Infrequent handwashing and inadequate surface disinfection can contribute to outbreaks of respiratory illnesses, including bronchiolitis.
Parents and caregivers should remain alert to the symptoms of bronchiolitis and seek medical attention if a baby shows signs of breathing difficulty, such as rapid breathing, wheezing, chest retractions (skin pulling in between the ribs or under the breastbone during breathing), or a bluish color around the mouth.
Prevention is key and includes good hand hygiene, avoiding exposure to tobacco smoke, and in some cases vaccination or preventive treatment (such as protection against respiratory syncytial virus for high-risk infants) to help protect this vulnerable population.
Home care for bronchiolitis
It is not always necessary to see a healthcare professional when bronchiolitis is mild, although with babies it is understandable to want medical advice. As a home-visit pediatric pulmonologist, these are the main measures I recommend to parents when bronchiolitis is mild and can be managed at home:
Maintain good hydration: offer feeds more frequently but in smaller amounts if the baby becomes tired while feeding.
Clear the airways: nasal saline washes help reduce congestion, especially before feeds.
Humidify the environment: using a cool-mist humidifier can help relieve mucus and coughing.
Monitor feeding and behavior changes: be alert if the baby tires easily during feeds or has fewer wet diapers than usual.
Manage fever or discomfort with antipyretics (only as advised by the pediatrician), in babies who are above the minimum recommended age and have no contraindications.
Avoid tobacco smoke and ensure good ventilation.
Many parents ask about using cough syrups or antibiotics “just in case.” In bronchiolitis, antibiotics are not routinely recommended, nor are most specific drug treatments, unless clearly indicated by a doctor.
When should you seek help from a pediatric pulmonologist for bronchiolitis?
You should seek immediate medical attention or go to the emergency department if you notice any of the following signs, as they may indicate a serious condition in your baby:
Severe breathing difficulty: Pay close attention to signs such as marked chest retractions (deep pulling in between the ribs and below the chest with each breath) or very fast, shallow breathing. These indicate that the baby is making a significant effort to breathe.
Changes in skin color: If the baby’s lips or fingernails turn bluish or grayish, this is a sign of cyanosis, meaning the baby is not getting enough oxygen. This is a medical emergency.
Feeding difficulties or altered level of alertness: If the baby cannot tolerate feeds, drinks very small amounts of milk, or is unusually sleepy and difficult to wake, this may indicate dehydration or a more serious illness.
Signs of dehydration: The number of wet diapers is a key indicator of hydration. Very few wet diapers over a 24-hour period is a warning sign of possible dehydration.
Apnea: Any pauses in breathing (apnea), especially if they are prolonged or recurrent, require urgent medical attention.
Worsening condition or new symptoms: If the baby’s overall condition worsens instead of improving, or if new and concerning symptoms appear, a medical evaluation is essential.
These situations are particularly concerning and require specialized medical assessment. Early intervention is crucial, as the baby may need treatments such as supplemental oxygen, intravenous fluids to correct dehydration, or even hospital observation for continuous monitoring and appropriate management.
Bronchiolitis and other respiratory infections can progress rapidly in infants and young children, making close observation and prompt response essential.
