Toe Walking in Children: What It Means, When It Is Normal and When to Seek Medical Advice

Dr. Fátima Olalla, pediatric neurologist
It is common for parents to notice their children walking on their toes. In many cases, this is a temporary gait pattern that forms part of normal development when a child is learning to walk. In fact, it can be considered a physiological variant until around 2–3 years of age, and it may be observed more frequently in children who were born prematurely.
However, if this pattern persists beyond that age or is associated with other clinical signs, a specialized evaluation may be recommended. It is usually assessed by pediatric orthopedics, specialists in motor development, and in some cases also by pediatric neurology, to rule out neurological or neurodevelopmental causes such as spasticity, proprioceptive or vestibular system disorders, or certain neurodevelopmental conditions in which toe walking may appear as a stereotyped behavior.
What does toe walking mean?

Created with GIMP
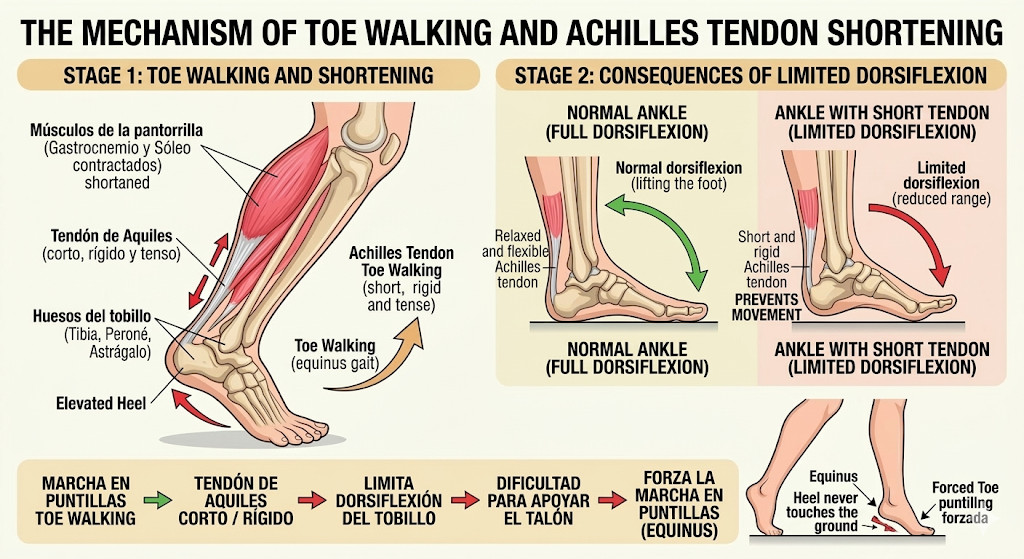
Toe walking (placing most of the body weight on the forefoot or the tips of the feet so that the heel does not touch the ground while walking) is common and often temporary in young children between 12 and 18 months, usually resolving before the age of two.
If this pattern persists after the age of three, becomes exclusive, or is associated with warning signs (such as unilateral toe walking or progressive worsening), it requires evaluation. It is generally classified into three types:
Idiopathic or habitual toe walking
This is the most common form and has no identifiable underlying cause. It is often considered a habit, sometimes with a family history, and the child can usually place the heel on the ground if asked.
Even when idiopathic and without warning signs, persistent toe walking should be monitored. If the habit continues and calf muscles are not properly stretched, it may eventually lead to tightness or shortening of the calf muscles and Achilles tendon.
Persistent idiopathic toe walking can lead to functional shortening of the calf muscles and Achilles tendon, which is why early monitoring and evaluation (by a pediatrician, neurologist, or physiotherapist) are important. Management may include observation, physiotherapy, orthoses, or, rarely, surgery.
Secondary to neurological conditions
Examples include:
Spastic cerebral palsy
Autism spectrum disorder
ADHD
Secondary to orthopedic conditions
Toe walking may occur due to anatomical shortening of the Achilles tendon or ankle stiffness, which prevents proper heel contact with the ground.
Is it normal for a child to walk on their toes?
Many toddlers between 12 and 18 months walk on their toes after they begin walking. This is usually part of motor exploration and does not necessarily indicate a problem.
Children experiment with balance and posture, and this gait pattern often resolves spontaneously as they gain stability and coordination.
The typical heel-to-toe gait pattern usually becomes established between 22 and 36 months (around 3 years of age). If toe walking persists beyond this age without other warning signs, it may be idiopathic toe walking, although pediatric or physiotherapy evaluation is recommended.
Idiopathic toe walking refers to a persistent gait pattern without detectable physical, neurological, or sensory causes.
Possible causes of toe walking
Although often harmless, toe walking may sometimes be associated with other conditions.
Motor development and habit
Children may continue an early motor pattern simply out of habit and repetition, even after more efficient walking patterns develop.
These habits are usually benign and resolve as the child matures, although evaluation may be advisable. Persistent idiopathic toe walking may eventually lead to muscle tightness or spasticity if not addressed.
Short Achilles tendon or tight calf muscles
A shortened or tight Achilles tendon limits ankle dorsiflexion, making it difficult for the heel to touch the ground and leading to toe walking.
This adaptation may temporarily relieve tension but can lead to:
Muscle overload: fatigue, pain, and increased risk of calf tendinopathies
Postural changes: misalignment from the foot up to the spine
Abnormal joint development in children
Increased shoe wear
Early detection by a specialist is essential to begin treatment such as stretching exercises, physiotherapy, or surgery in severe cases.

Neurological or developmental conditions
Persistent or asymmetric toe walking (beyond two to three years of age) requires medical and neurological evaluation because it may be associated with conditions affecting motor control.
Possible underlying causes include:
Cerebral palsy, particularly spastic forms affecting calf muscle tone
Autism spectrum disorder, possibly related to sensory processing differences or repetitive behaviors
Other conditions, such as developmental coordination disorder, myopathies, or atypical sensory processing
It is important to distinguish these from idiopathic toe walking, where development is otherwise normal.
Early intervention (physiotherapy, orthoses, etc.) helps improve function and prevent complications such as Achilles tendon shortening.
Another abnormal gait pattern sometimes seen is the waddling or “duck-like” gait, caused by weakness in the hip abductors (such as the gluteus medius).
Other associated findings may include:
Difficulty initiating or maintaining walking due to fatigue
Gowers’ sign, indicating proximal muscle weakness
Occasional toe walking
Although less common than neurological causes, atypical gait combined with proximal muscle weakness should raise suspicion of underlying muscular disease.
When should you be concerned?
It is advisable to consult a healthcare professional if:
The child continues toe walking after 2–3 years of age
There is marked ankle or Achilles tendon stiffness and the child cannot place the heel down even when asked
Other clinical signs are present, such as motor delays, frequent falls, pain, or limited mobility
The gait pattern changes over time, especially if the child previously walked heel-to-toe
Toe walking occurs only on one side
Early evaluation can help rule out musculoskeletal, neurological, or sensory conditions and establish a management plan if necessary.
How is it clinically evaluated?
A specialist in pediatric orthopedics or pediatric rehabilitation performs a comprehensive evaluation of the child’s musculoskeletal system and motor function.
The consultation usually focuses on three key aspects:
Gait and foot support assessment
The specialist observes the walking pattern (limping, toe walking, rotation) and the footprint pattern, checking for flat feet, high arches, or asymmetries.
Flexibility and muscle tone examination
The flexibility of the Achilles tendon (dorsiflexion) and the child’s overall muscle tone and strength are assessed.
Detection of neuromuscular signs
The doctor evaluates reflexes, asymmetries, and developmental milestones that could suggest neurological or muscular disorders.
Individualized management plan
Management may include:
Periodic observation for mild cases or normal developmental variations
Therapeutic exercises at home, including stretching and strengthening
Physiotherapy or occupational therapy, sometimes with orthoses or supportive devices
Treatment usually begins with observation and follow-up, as many children improve naturally with growth and maturation. In selected cases, physiotherapy, orthotic devices, splints, or casting may be used.
If an underlying neurological or musculoskeletal condition is identified, treatment will be personalized and multidisciplinary.
Pediatric orthopedic evaluation at home in Madrid
We understand that traveling with a child can be difficult, especially when gait problems cause instability or discomfort.
At drarebeccaordovas.com, we offer pediatric orthopedic and pediatric neurology home evaluations in Madrid, where a specialist can:
Observe the child’s gait in their natural environment
Perform a complete musculoskeletal examination
Provide personalized recommendations and exercises
Idiopathic toe walking is usually diagnosed through a clinical evaluation by both a pediatric orthopedic specialist and a pediatric neurologist, without the need for additional tests.
Once pathological causes are ruled out, early detection and intervention are essential. This may include home stretching exercises performed by parents or physiotherapy to prevent complications such as muscle tightness or spasticity.
This personalized approach is ideal for families who prefer a calm, comfortable assessment aligned with the child’s daily routine.
